Jose Meade Aguilar, an Internal Medicine resident at Boston University, dives into the ANDROMEDA-SHOCK trial. He compares capillary refill time (CRT) to lactate-guided resuscitation in septic shock, highlighting CRT's advantages as a rapid assessment tool. The trial's aim and multicenter design are outlined, with a focus on the patient demographics and measuring techniques used. While the results showed an 8.5% mortality difference favoring CRT, it wasn't statistically significant. Jose also emphasizes the practical use of CRT in clinical settings.
20:08
forum Ask episode
web_stories AI Snips
view_agenda Chapters
auto_awesome Transcript
info_circle Episode notes
insights INSIGHT
CRT Is A Fast, Practical Perfusion Marker
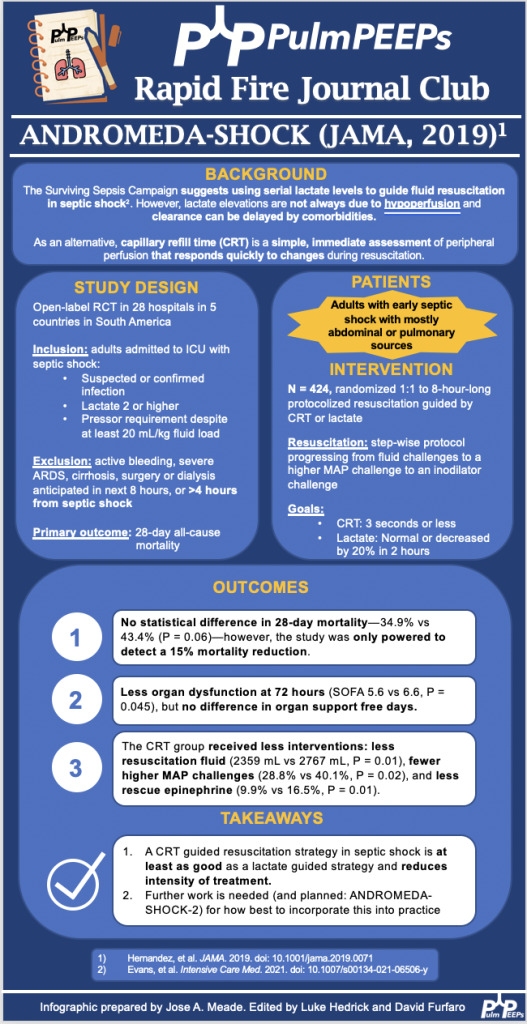
Capillary refill time (CRT) is a rapid, low-cost measure that reflects peripheral perfusion and responds quickly to resuscitation changes.
Lactate can be elevated for nonhemodynamic reasons and may clear slower, limiting its bedside responsiveness.
We are excited to be back with a Rapid Fire Journal Club. Today’s episode is hosted by PulmPEEPs Associate Editor, Luke Hedrick, and will delve into the ANDROMEDA-SHOCK trial published in JAMA in 2019.
Meet our Guests
Jose Meade Aguilar is a second year Internal Medicine resident at Boston University Medical Campus (BUMC).
Article and Reference
Today the discussion highlights the ANDROMEDA-SHOCK trial (JAMA, 2019) which evaluated whether resuscitation guided by capillary refill time (CRT) is superior to lactate-guided resuscitation in reducing mortality in patients with septic shock.

 PulmPEEPs
PulmPEEPs