Dr. Mark Creager, Professor of Medicine at Dartmouth Hitchcock and lead author of the 2026 multisociety pulmonary embolism guideline, walks through the new guideline framework. He explains the new A–E clinical categories and respiratory modifiers. The conversation covers updated risk assessment, diagnostic approaches including imaging and D-dimer use, role of echocardiography, anticoagulation choices, advanced therapies, and follow-up strategies.
00:00
forum Ask episode
web_stories AI Snips
view_agenda Chapters
auto_awesome Transcript
info_circle Episode notes
insights INSIGHT
New A–E PE Clinical Categories
The new A–E clinical categories create a severity continuum replacing massive/submassive and low/intermediate/high labels.
Category C subdivides into C1–C3 by RV function and biomarkers, while D and E capture incipient and frank cardiopulmonary failure with respiratory modifiers for hypoxia.
volunteer_activism ADVICE
Start With Clinical Probability And D-dimer
Begin PE evaluation with history, exam, and validated clinical probability tools like Wells, revised Geneva, and PERC.
If clinical probability is low and D-dimer is normal, avoid imaging; otherwise proceed to imaging for confirmation.
volunteer_activism ADVICE
Prefer CTPA Then VQ-SPECT If Contraindicated
Use CTPA as the preferred diagnostic imaging for suspected PE when available and no contraindication exists.
If CTPA is contraindicated, prefer VQ-SPECT over planar VQ because it has better specificity and reproducibility.
Get the Snipd Podcast app to discover more snips from this episode
We are unbelievably excited this week to be reviewing the hot-off-the-presses 2026 Multi-Society (AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN) Pulmonary Embolism Guidelines with lead author Dr. Mark A. Creager. We will talk about key updates in these guidelines compared to prior practice, including the new risk classification model, and provide an overview from diagnosis to follow-up. Given the clinical importance and prevalence of pulmonary embolism, these guidelines are certainly going to shape practice going forward, so this episode is a can’t miss!
Watch the full video of this episode with graphics and helpful teaching visuals on our YouTube channel: https://www.youtube.com/@pulmpeeps
Meet Our Guest
Dr. Mark Creager is a Professor of Medicine at Dartmouth Hitchcock Medical Center where he specializes in Cardiovascular Medicine with an emphasis on venous thromboembolic disease. He served as the lead author of the 2026 Pulmonary Embolism Guidelines.
This is the first joint AHA/ACC clinical practice guideline specifically on acute PE, bringing together a truly multidisciplinary writing committee (cardiology, pulmonology, hematology, emergency medicine, interventional radiology, surgery, and others). Prior guidelines existed from individual societies, but nothing this comprehensive had been updated in roughly five to six years.
New PE clinical categories (A through E):
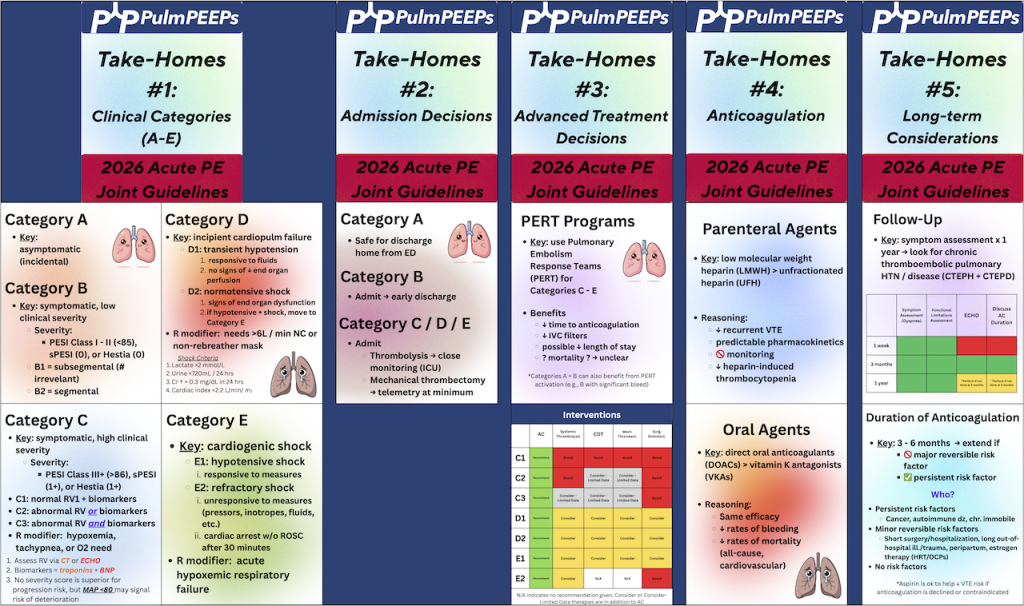
One of the most impactful changes is replacing the old “massive/submassive” and “low/intermediate/high risk” labels with five categories that form a severity continuum. Category A is subclinical (incidental PE found on imaging in asymptomatic patients). Category B covers symptomatic but low-severity patients. Category C is where much of the clinical complexity lives — symptomatic, hemodynamically stable patients subdivided into C1, C2, and C3 based on RV function and biomarkers. Category D represents incipient cardiopulmonary failure (transient hypotension, normotensive shock with end-organ dysfunction). Category E is frank cardiopulmonary failure, with E2 being the sickest — refractory or recurrent cardiac arrest. Respiratory modifiers (hypoxia requiring supplemental oxygen) layer onto C, D, and E.
Diagnostic approach:
Clinical evaluation comes first — history, exam, and validated decision tools (Wells score, revised Geneva, PERC). If clinical probability is low and D-dimer is normal, imaging can be safely avoided. If either is concerning, imaging is warranted. CTPA remains the preferred imaging modality due to superior sensitivity, specificity, wide availability, and ability to assess clot burden and alternative diagnoses. VQ scanning is still appropriate when CTPA is contraindicated, and VQ SPECT offers better reproducibility and specificity than traditional planar VQ if available. Echocardiography is not a diagnostic test for PE but is important for risk stratification — RV size, TAPSE, and tissue Doppler measures all contribute prognostic information.
Anticoagulation updates:
Anticoagulation remains the cornerstone of treatment. For patients potentially needing advanced therapies (C3, D, E), parenteral anticoagulation is started first. A notable recommendation: low molecular weight heparin is generally preferred over unfractionated heparin, based on evidence showing more effective VTE risk reduction, more predictable pharmacokinetics, no need for routine monitoring, lower rates of heparin-induced thrombocytopenia, and no increase in major bleeding. The committee acknowledged this may create discomfort for clinicians accustomed to unfractionated heparin’s easy reversibility, but the difficulty of achieving and maintaining therapeutic levels with UFH was a significant concern.
Advanced therapies:
Catheter-based thrombolysis, mechanical thrombectomy, systemic thrombolysis, and surgical embolectomy all received mostly class 2B recommendations (“can consider”) for C3 and D categories, reflecting that current evidence shows improvement in short-term surrogate measures (RV/LV ratio, hemodynamics) but lacks definitive hard outcome data on mortality. For category E1 patients, recommendations are stronger (class 2A). Multiple trials are expected soon — HI-PEITHO, PEERLESS-2, PE-TRACT, PERSEVERE, TORPEDO, and PROG — that should substantially inform future updates.
PERT teams:
Pulmonary embolism response teams are encouraged, particularly for C3, D, and E patients. They’ve been shown to reduce length of stay. For institutions without PERT capability, establishing consultation networks with larger centers is recommended.
Post-PE follow-up:
Patients shouldn’t be “left in the wilderness” after discharge. The guidelines recommend communication within the first week to ensure understanding of diagnosis and treatment, an in-person visit at or before three months to assess for persistent symptoms and discuss anticoagulation duration, ongoing surveillance for chronic thromboembolic pulmonary disease, and periodic reassessment for those on extended anticoagulation.

 PulmPEEPs
PulmPEEPs