Dive into the complexities of Acute Respiratory Distress Syndrome (ARDS) as this discussion launches a summer series on landmark trials. Explore the impactful ARMA trial, which revolutionized ventilation strategies in ARDS care by comparing traditional and lower tidal volumes. Discover how participant selection and trial methodologies shape critical outcomes like mortality and vent-free days. The episode emphasizes lung-protective ventilation practices, the evolution of pulmonary care, and the implications for personalized treatment approaches.
17:40
forum Ask episode
web_stories AI Snips
view_agenda Chapters
auto_awesome Transcript
info_circle Episode notes
insights INSIGHT
ARMA Trial Changed ARDS Ventilation
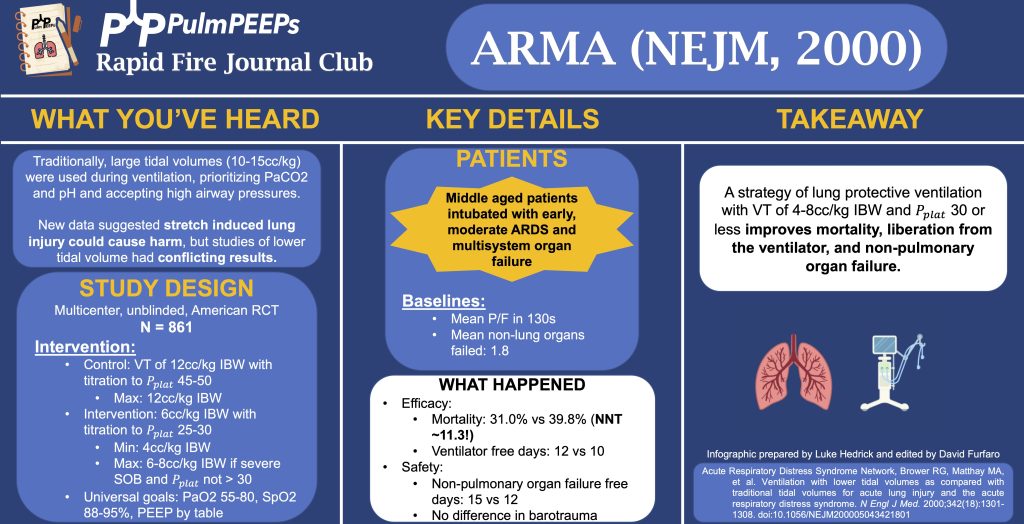
The ARMA trial compared ventilation strategies in ARDS, fundamentally changing standard care.
It established lower tidal volumes and plateau pressures significantly improve outcomes.
insights INSIGHT
Tidal Volume Strategies Compared
The trial compared high tidal volumes (~12 cc/kg) against low volumes (~6 cc/kg) with plateau pressures of 30 or less.
Both groups used similar PEEP and oxygenation targets to isolate tidal volume effects.
insights INSIGHT
Positive Outcomes With Low Tidal Volumes
Lower tidal volume ventilation reduced mortality from ~40% to 31% and increased ventilator-free days.
The number needed to treat was just over 11, showing a strong benefit for lung protective ventilation.
Get the Snipd Podcast app to discover more snips from this episode
This episode is launching our 2024 Rapid Fire Journal Club summer series on ARDS! This summer we will be talking about landmark ARDS trials that have defined the literature and shaped patient care. Journal clubs often focus on new trials, and so learners may have a less thorough understanding of the baseline literature that defines many of our ICU practices. The goal of this series is to provide a quick, but in-depth look at these papers so that learners understand the modern landscape of ARDS.
We’re talking about the ARMA trial today which examined “Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome.”
We mention a step-wise titration of tidal volume in the control group to achieve Pplats of 45-50. To clarify, there was no adjustment of Vt in the traditional Vt group unless Pplat > 50. If Vt had been decreased in the traditional Vt group because Pplat was > 50, it would not be subsequently increased back to 12 unless Pplat < 45 (to avoid a cycle of corrections and re-adjustments). Similarly in the lower Vt group, there was no adjustment (“titration”) of Vt unless Pplat > 30, and there was a similar protocol in place not to increase the Vt again unless the Pplat was < 25.

 PulmPEEPs
PulmPEEPs